
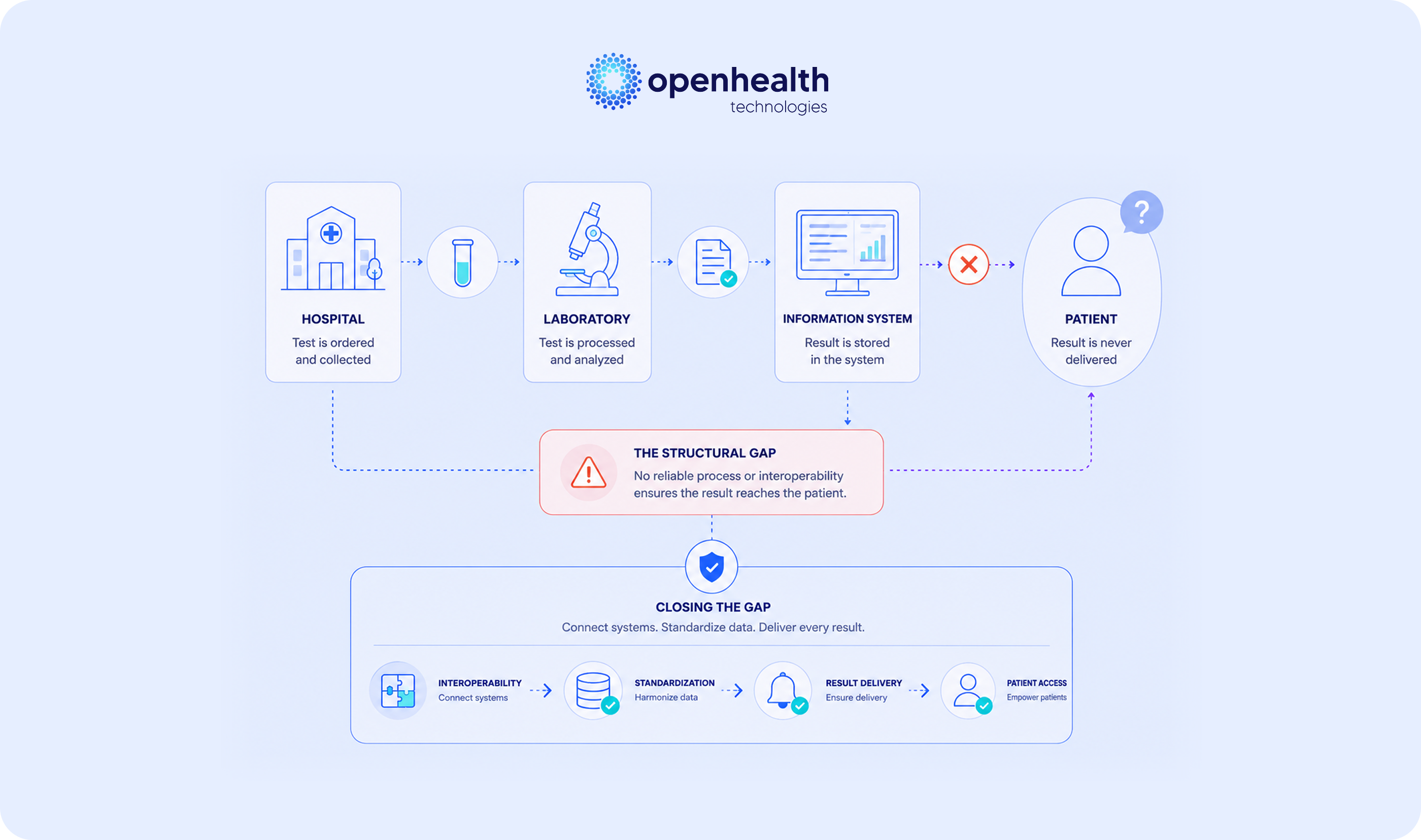
During a typical inpatient stay at a Brazilian general hospital, a patient may undergo dozens of laboratory tests, ranging from complete blood counts and basic biochemistry to hormonal assays, inflammatory markers, serologies, and organ function tests. These data feed clinical decisions that occur within short timeframes, are recorded in the hospital chart, and at discharge they remain where they were recorded: in the hospital chart. The patient receives a discharge summary with narrative text and, occasionally, a few printed reports they specifically requested. The structured set of laboratory data the hospital produced about the patient's own body remains, in practice, inaccessible to them. This arrangement is so naturalized it is rarely discussed for what it actually is: a structural failure in returning data the patient has the right to receive.
What the LGPD says and what the patient receives
Brazil's General Data Protection Law (Lei nº 13.709/2018) classifies health data as a special category of sensitive personal data and establishes, in Article 18, the data subject's right to obtain confirmation of existence and access to their data from the controller upon request.¹ This right is not abstract. It applies directly to clinical data produced during hospital admissions, including laboratory results.
In practice, exercising this right faces operational friction that hollows out its purpose. Patients who request a copy of their hospital chart usually receive physical documents, or PDF files reproducing the clinical document but containing no structured data. The lab report that existed in structured form within the hospital's Laboratory Information System reaches the patient as image of text: human-readable, but not comparable, not integrable, and not actionable on any platform that depends on structured data.
Brazil's National Data Protection Authority intensified in 2024 and 2025 its oversight of health data processing practices, with growing focus on transparency, right of access, and portability.² The regulatory landscape is moving toward requiring that data return to the data subject occurs in a format that effectively enables exercise of their rights, not in a format that formally meets the requirement without enabling practical use of the information.
The clinical cost of unstructured delivery
The consequence of unstructured delivery goes beyond regulatory compliance. It carries measurable clinical impact.
Patients discharged from hospital then enter an outpatient care phase conducted by physicians different from those who treated them as inpatients. The cardiologist who will follow up after an admission for acute heart failure ideally needs access to troponin, BNP, renal function, and electrolyte curves during admission. The endocrinologist taking over after a diabetic decompensation admission needs the time series of blood glucose, HbA1c, and renal function measured in the hospital. When these data reach the outpatient physician as a PDF discharge summary, with no structure, no comparable time series, no standardized nomenclature, continuity of care depends on manual reconstruction of information, frequently incomplete.
Research on inter-level care communication has identified that failures in clinical information transfer between hospital and outpatient care are documented causes of adverse events, readmissions, and test duplication.³ The World Health Organization recognizes that failures in clinical information communication, including laboratory results, are among the leading causes of preventable adverse events in healthcare.⁴ The patient who leaves the hospital without structured access to their own laboratory data is, in practical terms, a patient whose continuity of care begins with an informational deficit.
What changes with the RNDS
Brazil's Ministry of Health published Ordinance GM No. 8,276 in October 2025, establishing the Laboratory Test Result Information Model (REL) within the National Health Data Network (RNDS).⁵ The ordinance requires that laboratory results from across the national territory follow defined standards, with LOINC terminologies or the codification adopted in GAL, and be sent regularly to RNDS. The regulatory direction is clear: laboratory data must exist in structured, interoperable form, accessible to the national digital health infrastructure.
The logical consequence for the hospital ecosystem is direct. Hospitals that meet the RNDS submission obligation will, by construction, be producing laboratory data in structured and interoperable form. There is no technical justification for that same data, already existing in adequate format, not being made available to the patient who originated it. The barrier ceases to be technological and becomes process-based: the hospital decision to deliver or not deliver data in structured form to the patient.
Brazil's Letter of Health User Rights, established by the Ministry of Health, already recognized the user's right to access their clinical history.⁶ The LGPD reinforced this right with statutory force. The RNDS solves the technical part. What remains is the hospital decision to treat structured data return as a strategic element, not as operational burden.
The competitive dimension of structured return
For hospitals and hospital networks, structured return of laboratory data to the patient has stopped being only legal compliance. It has become an element of perceived quality and competitive differentiation in a segment where the dispute over patient acquisition and retention intensifies year over year.
Patients who receive from the hospital a structured return of their laboratory data, integrable to personal health applications and accessible to their outpatient physician in a format comparable to data produced at other providers, perceive the hospital as a provider that respects their informational autonomy. Studies on patient satisfaction in hospital settings identify transparency and access to information among the attributes with strongest correlation to recommendation and loyalty.⁷ In a context where the commoditization of physical infrastructure and analytical technical capacity reduces space for traditional differentiation, the way the hospital treats the information it produced about the patient becomes, itself, a vector of differentiation.
The discussion about patient experience in hospitals usually concentrates on hospitality, waiting time, and humanized care. These elements matter. But there is a less obvious and increasingly decisive dimension: how the patient takes with them, on leaving, the clinical information the hospital produced about their own body. Hospitals that treat this delivery with the same seriousness they treat clinical care quality are building a loyalty asset that doesn't depend on price reduction or additional infrastructure investment.
From obligation to asset
Structured return of laboratory data to the patient is not a standalone project. It is a natural extension of the data infrastructure the hospital needs to build to meet regulatory obligations and operate with internal efficiency. The same data that needs to be harmonized to feed the chart, the billing system, the RNDS, and decision-support algorithms can be made available to the patient in equally structured form, at near-zero marginal cost, when the semantic harmonization layer is in place.
This is where OpenHealth Technologies operates. The platform automatically correlates multiple data streams with rigorously validated logical layers of laboratory tests, delivering laboratory data in semantically coherent structure, mapped to LOINC, longitudinally comparable, and exportable in formats that serve both RNDS integration and patient return. For hospitals and hospital networks, this means the layer that sustains regulatory compliance is the same that enables structured delivery to the patient, without duplicated effort and with full leverage of the data infrastructure investment.
Learn how your institution can transform hospital laboratory data into structured patient return, expanding compliance and competitive differentiation.