
Fifty million Brazilians have private health insurance.¹ The other 160 million depend exclusively or primarily on the Unified Health System (SUS). But this division, which appears binary in aggregate numbers, is far more porous in practice: patients move between the two systems throughout their lives as their employment, income, city of residence, or health status changes. They lose their plan, return to SUS. Gain coverage, migrate to private. Have routine tests at the public health unit and specialized procedures at private clinics.
Brazil's health system, in practice, is hybrid. The laboratory data it generates is not.
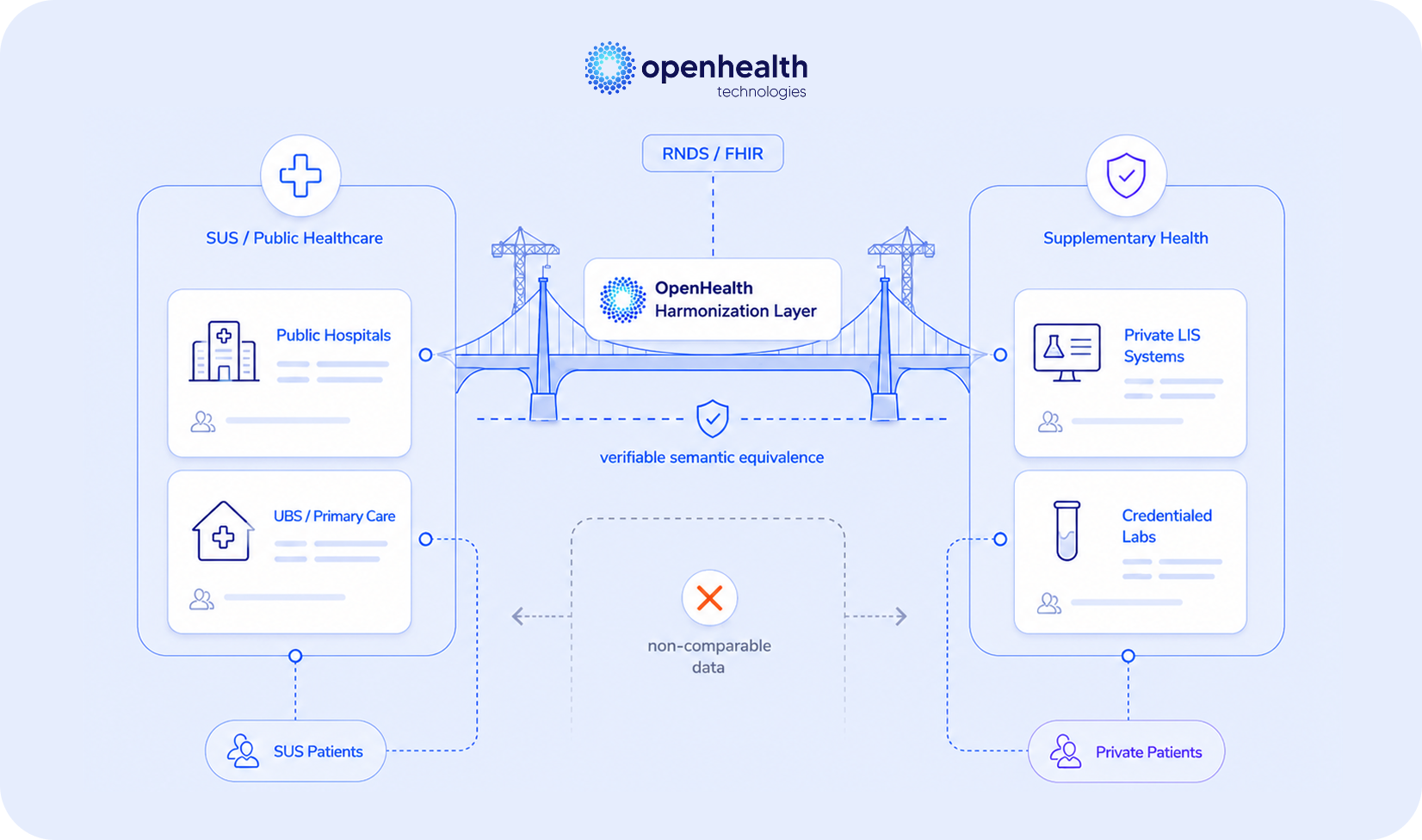
Two systems, two languages, one patient
The SUS laboratory network operates under distinct architectures depending on the type of service. The Central Public Health Laboratories (LACENs) and the epidemiological surveillance network use the Laboratory Environment Manager (GAL), a platform developed by DATASUS in partnership with the General Coordination of Public Health Laboratories (CGLAB), designed to manage surveillance tests and compulsory notification diseases.² Routine clinical laboratories linked to primary health units, public hospitals, and municipal credentialed services operate, in practice, on a variety of systems, some proprietary, many legacy, with heterogeneous standardization across states and municipalities. The private network runs on dozens of different commercial LIS systems, each with its own nomenclatures, code tables, and reference ranges.
The two ecosystems were built with independent logic, operate under different rules, and in almost all cases, do not communicate with each other.
The result is that a patient who has had five years of routine tests in the public system, with semi-annual blood counts, annual fasting glucose, and lipid panel, and who acquires a private health plan, starts for all practical purposes from zero in the private system. The physician who sees them in their first private consultation has no structured access to the laboratory history produced by the SUS. They may ask the patient to bring paper reports or PDFs, but these documents preserve the format and destroy the semantics.³ They are not comparable data. They are images of text.
The reverse situation is equally common. A patient who loses their job and with it their corporate health plan returns to SUS with a laboratory history produced by private laboratories that the public system cannot incorporate in structured form. The biomarkers that had been monitored in the private sector must be reestablished as if from scratch, without the trajectory that gave them their clinical meaning.
Discontinuity as a measurable clinical risk
Laboratory data discontinuity in the transition between systems is not merely an administrative inconvenience. It has documented clinical impact, especially for patients with chronic diseases, precisely the profile that most frequently moves between the two systems, as it is also the one that most uses health services.
When a physician lacks access to a chronic patient's prior laboratory trajectory, the practical consequences are predictable: ordering tests already performed to reestablish a baseline, inability to evaluate trends in critical biomarkers such as creatinine, HbA1c, and TSH, and greater likelihood of therapeutic decisions based on insufficient data. Studies on care fragmentation show that patients without clinical information continuity have higher hospitalization rates, more emergency consultations, and poorer control of chronic conditions.⁴
The problem has scale. Brazil recorded more than 2.5 billion laboratory tests in 2024, of which 53.6% in the SUS and 46.4% in the private network.⁵ A significant portion belongs to patients who move between the two systems. Each transition without semantic data continuity represents a rupture in that patient's clinical timeline, a rupture that appears in no quality indicator, but that has real impact on the decisions that will be made at the next consultation.
What regulation already requires, not what it will require
In October 2025, the Ministry of Health published Ordinance GM No. 8,276, which establishes the Laboratory Test Result Information Model (REL) within the National Health Data Network (RNDS).⁶ The ordinance is direct: laboratory test results from across the entire national territory must follow the defined standards and be sent regularly to RNDS. Required terminologies are LOINC or the coding adopted in GAL. Electronic signature is mandatory.
This changes the framing of the interoperability discussion in Brazil. The question is no longer whether laboratory data will need to be structured and sent to RNDS. It is how and when each laboratory will comply with an obligation already in force. Laboratories, diagnostic networks, and hospitals that have not yet mapped their data to LOINC or GAL coding are, as of October 2025, out of compliance with a Ministry of Health regulatory requirement.
The REL model defines the mandatory fields of the test result that must be transmitted to RNDS, including standardized terminology, reference ranges, analytical methodology, patient metadata, and electronic signature. These are exactly the fields that, in most Brazilian laboratories, exist in incomplete, inconsistent, or unstructured form. The ordinance didn't create a new problem. It articulated in regulatory language a data infrastructure problem that already existed.
The RNDS, originally regulated by Ordinance No. 1,434/2020 and now with the REL model defined, represents the backbone of public-private interoperability that Brazil's health system has always needed.⁷ When fully implemented, a laboratory result produced by a SUS-credentialed lab in Belém will be accessible, in structured form, to the physician seeing the same patient at a private clinic in São Paulo, and vice versa. The patient's clinical timeline ceases to belong to the system that generated it and begins to belong to the patient.
The opportunity in compliance
The publication of Ordinance 8,276 transforms what until October 2025 was a strategic advantage into a regulatory requirement. But the distinction between those who comply now and those who will wait for enforcement is real, and has competitive consequences.
Laboratories and diagnostic networks that invest now in semantic harmonization, with LOINC mapping, documented reference ranges, and complete clinical metadata structured for RNDS submission, will make the transition with room to test, correct, and refine before enforcement mechanisms operate at scale. Those who wait will make the same transition under pressure, with operational risk and without the learning window that early adoption allows.
There is also a gain that goes beyond compliance. A laboratory operating with semantically structured data compatible with RNDS/LOINC doesn't only fulfill the ordinance. It builds infrastructure that enables uses well beyond the regulatory obligation: integration with institutional clients' health systems, chronic disease management programs, population health initiatives, and, in the medium term, access to structured data markets that depend exactly on this quality layer.
This is the context in which OpenHealth Technologies is positioned. The platform automatically correlates multiple data streams with rigorously validated logical layers of laboratory tests, with native LOINC mapping covering more than 3,500 biomarkers. For laboratories that need to align their data with the RNDS REL model, this means the semantic harmonization layer, the central technical requirement of the ordinance, is already built. For networks operating in both ecosystems, public and private, it means data produced at any point carries verifiable clinical equivalence and is structured to meet both Ordinance 8,276 and the integrations that RNDS will progressively enable.
Learn how your institution can ensure compliance with the RNDS REL model and clinical continuity of laboratory data between public and private health systems.