
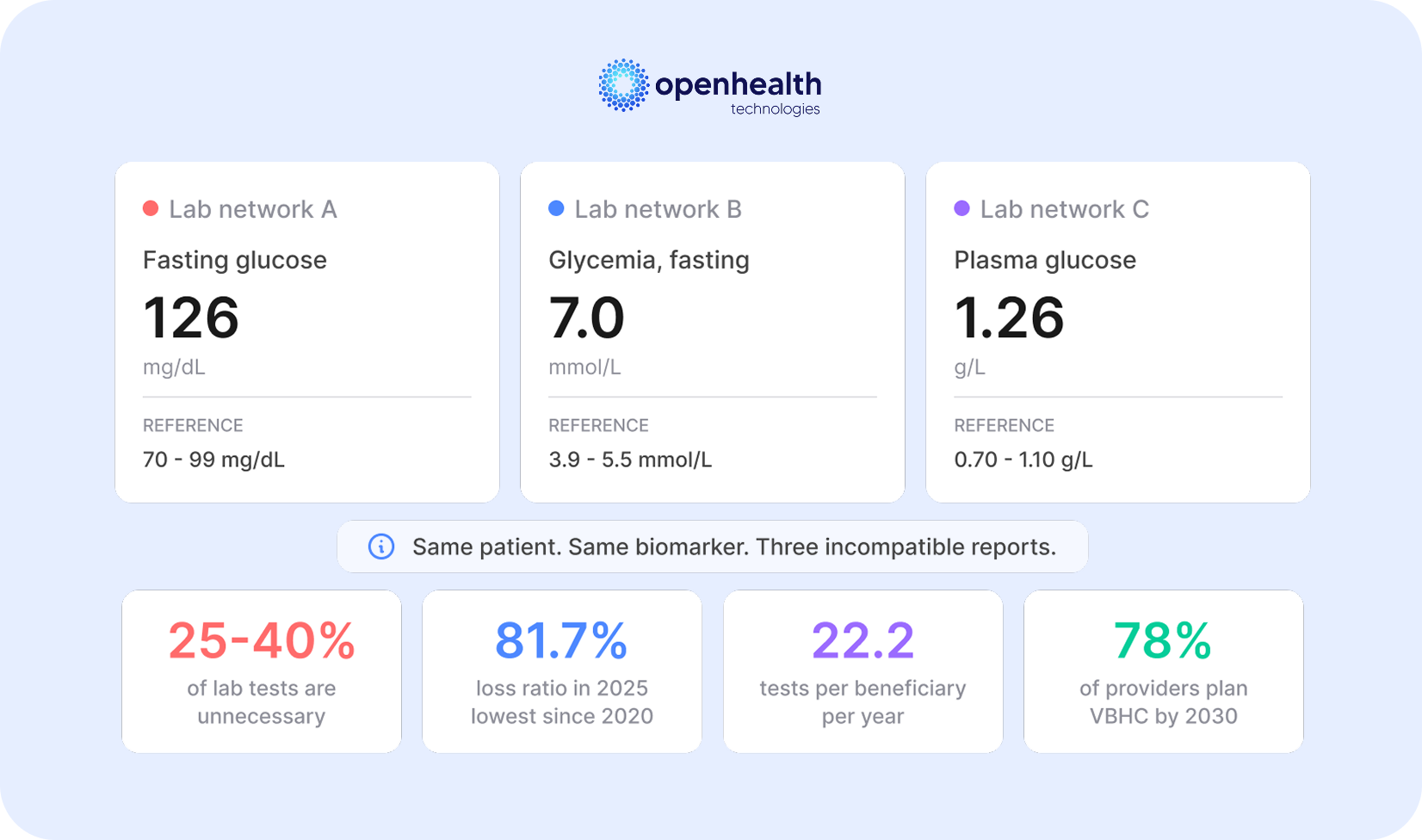
Between 25% and 40% of laboratory tests performed in Brazil’s private health insurance system are unnecessary. In absolute terms, the Institute for Supplementary Health Studies (IESS) estimates this inefficiency represents over R$ 12 billion (US$2.4 billion) annually in waste, a figure that exceeds the individual budgets of hundreds of Brazilian hospitals and is silently absorbed by health insurers as an unavoidable operating cost. Brazil’s supplementary health sector closed 2025 with a loss ratio of 81.7%, the lowest since 2020, and a record net profit of R$ 24.4 billion. These figures may suggest a comfortable outlook. However, the reduction in the loss ratio was primarily driven by premium increases exceeding the growth in healthcare expenses, not by structural efficiency gains. The root cause of waste remains intact has a name: fragmented laboratory data.
When an insurer operates a credentialed network with dozens or hundreds of laboratories (each issuing reports with different nomenclatures, units of measurement, and reference ranges) comparing results becomes impossible. A blood glucose test recorded as “Fasting Glucose” in one lab, “Fasting Glycemia” in another, and “Plasma Glucose” in a third, with varying units and reference ranges, cannot be analyzed longitudinally or cross-referenced without manual intervention. The operational impact of this fragmentation is direct. Chronic disease management programs (diabetes, hypertension, and chronic kidney disease) depend on longitudinal biomarker analysis to monitor patient progression and adjust treatment plans. Without comparable data across credentialed laboratories, these programs operate with incomplete information, unable to identify trends, generate automated alerts, or reliably measure outcomes. For the insurer, this translates into lost clinical effectiveness and avoidable costs from hospitalizations and procedures that could have been prevented.
Fragmentation also fuels a well-documented phenomenon: the diagnostic cascade. Variations of just 10% in reference ranges between laboratories can trigger unnecessary follow-up tests in up to 30% of cases, generating consultations, procedures, and referrals to rule out non-existent pathologies. A study by researchers at Hospital de Clínicas de Porto Alegre and UFRGS found that in low-risk surgical procedures, 57.5% of patients underwent at least one unnecessary pre-operative test (95.3% of them laboratory tests) generating costs of R$ 10.88 million in the analyzed cohort alone. The predominant reimbursement model in Brazil intensifies the problem. Under the fee-for-service system, each procedure generates a payment to the provider regardless of clinical necessity or patient outcome. In 2022, each health plan beneficiary underwent an average of 22.2 tests, a rate higher than in previous years and significantly above OECD averages for high-complexity exams such as MRI.⁵ This growing volume occurs without effective mechanisms for verifying duplicates across providers, precisely because the data aren’t comparable.
The transition to value-based reimbursement models (Value-Based Healthcare — VBHC) is recognized by Brazil’s National Supplementary Health Agency (ANS) and the market as the path to sector sustainability. The agency has been promoting alternatives to fee-for-service since 2016, culminating in its Guide to Value-Based Reimbursement Models. According to a survey by the Brazilian Institute of Value in Health (IBRAVS) in partnership with L.E.K. Consulting, 78% of providers plan to expand value-based models by 2030. Yet implementing these models runs into a fundamental technical requirement: structured, comparable, and reliable laboratory data. The president of IBRAVS has publicly stated that without reliable, shared data, it’s impossible to pay for what truly matters: the clinical outcome. Only 10% of Brazilian hospitals have any contract effectively based on value, and the lack of integrated data is cited as one of the main barriers to expansion.
For insurers, the implication is clear: laboratory data infrastructure is a prerequisite for any serious strategy around loss ratio management, care coordination, or VBHC implementation. Without it, automated clinical alerts fire on inconsistent information, management dashboards display distorted indicators, and predictive models train on data that don’t reflect beneficiaries’ clinical reality. The lack of clinical data interoperability is estimated to represent between 8% and 15% of operating costs for a mid-sized health organization. For insurers managing networks with thousands of providers and millions of beneficiaries, this translates into hundreds of millions of reais wasted annually on rework, report reprocessing, manual data reconciliation, and missed opportunities for early intervention.
There is also a care quality dimension that directly impacts beneficiary perception. When a patient takes tests at different credentialed labs and finds that results don’t align — or when they need to repeat tests because a physician can’t compare previous reports — dissatisfaction with the health plan grows. Research shows that fragmented care is associated with more emergency visits and hospitalizations, driving up the loss ratio in the highest-cost segments.
The solution doesn’t lie in restricting access to tests or creating additional administrative barriers. It lies in ensuring that laboratory data generated by the credentialed network are harmonized: that results from different laboratories, methods, and instruments carry verifiable clinical and semantic equivalence. Harmonization isn’t merely standardizing technical formats, it’s ensuring that “Fasting Glucose” and “Fasting Glycemia,” measured by different methods and instruments, are clinically interpretable on the same scale and under the same reference criteria. This harmonization is what enables effective chronic disease management programs, automated detection of diagnostic cascades, real benchmarking across providers, and ultimately the transition to value-based reimbursement models. It is the infrastructure layer without which none of these initiatives can operate reliably.
It is within this context that OpenHealth Technologies stands out. The platform automatically correlates multiple data streams with rigorously validated logical layers of laboratory tests, ensuring not only technical connectivity but semantic integrity and clinical accuracy. For health insurers, this means transforming fragmented databases from credentialed laboratories into a unified, traceable, and clinically meaningful timeline: the foundation on which loss ratio management, care coordination, and VBHC programs can finally operate with the reliability the sector demands.
Learn how your organization can transform fragmented laboratory data into actionable clinical intelligence.